Focusing on the six outcomes we determined, PAP will continue to partner with DCFS, our Align Coalition, and the Little Rock faith organizations to build a prevention strategy and campaign action plan while integrating the insights gained from our geospatial analysis, psychographic segmentation analysis, and community focus group research and recommendations.
We will work with DCFS to acquire the remaining services, death, and ACES data needed to support our program methodology, ensuring the greatest impact.
Recommended evidence-based prevention for the six outcomes
Child Abuse and Neglect
- Reduces stigma around help-seeking
- Enhances connectedness to build resiliency in the face of adversity
- Fosters healthy and positive norms around gender, masculinity, and violence to protect against violence towards intimate partners, children, and peers
- Promotes safe and effective discipline
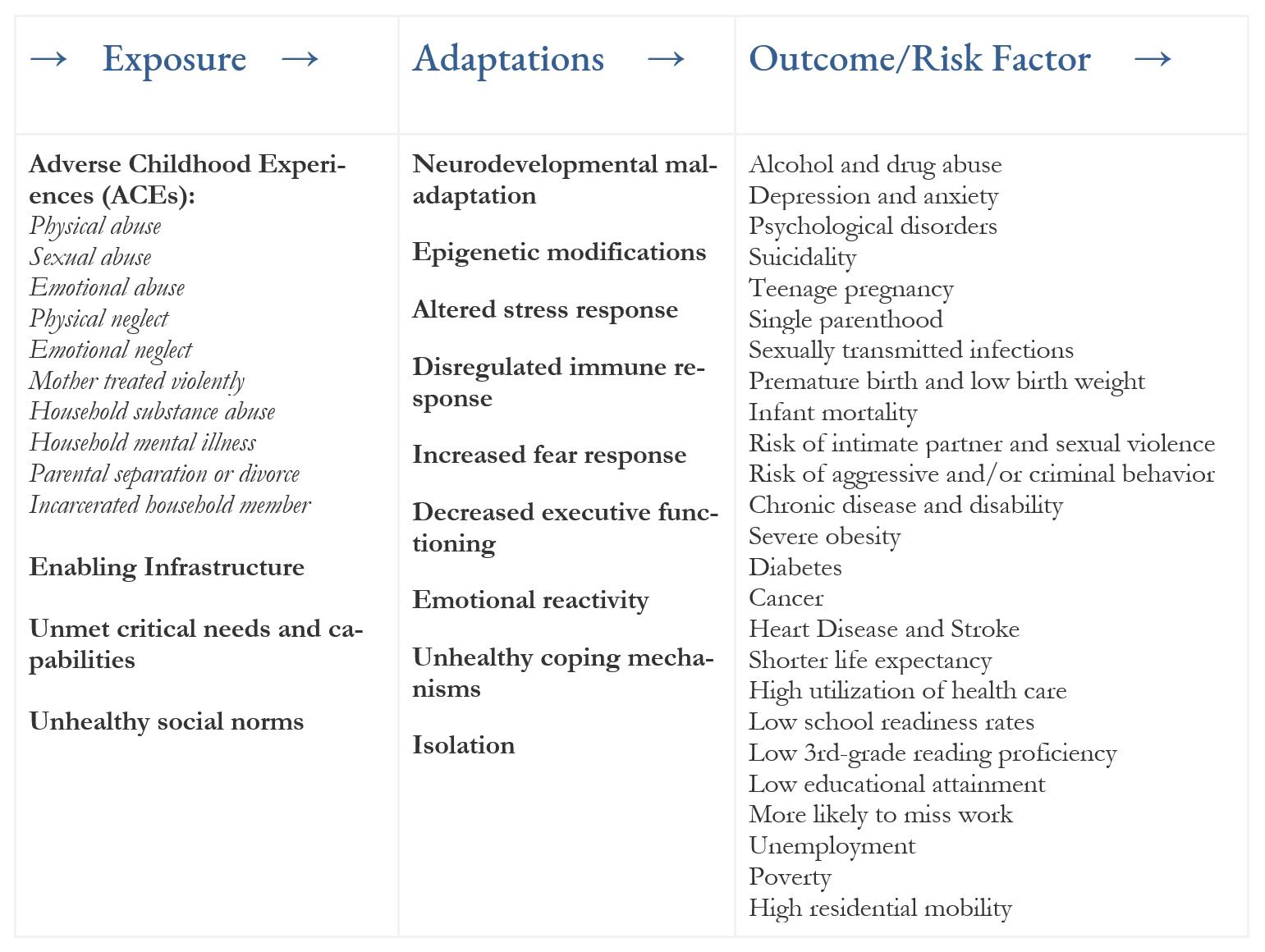
- Supports ACEs awareness
Infant mortality
- Provide childcare providers training in safe infant sleep practices
- Create and ensure existing messages in media depict safe sleep practices that are consistent with the American Academy of Pediatrics recommendations
- Expand parent education, training efforts, statewide regulations, mandates, and monitoring to decrease further risk of sudden infant death syndrome
- Train healthcare professionals to share the importance of folic acid intake before and during pregnancy
- Build public awareness around women of reproductive age needing 400 mcg of folic acid every day and how to ensure they receive enough in their diet
Suicide
- Increase access to mental health providers in underserved areas by expanding the reach of health services through telephone, video, and web-based technologies
- Create environments that address risk and protective factors where individuals live, work, and play include erecting barriers or limiting access to prevent jumping
- Educate on safe storage practices of medications, firearms, and other household products
- Encourage organizational policies and culture that promote protective environments such as prosocial behavior, skill-building, positive social norms, assessment, referral and access to helping services (e.g., mental health, substance abuse treatment, financial counseling) in places of employment, detention facilities, and other secured environments
- Address community-based policies to reduce excessive alcohol use such as zoning to limit the location and density of alcohol outlets, taxes on alcohol, and bans on the sale of alcohol for individuals under the legal drinking age
- Implement peer norm programs that seek to normalize protective factors for suicide such as help-seeking, reaching out to trusted adults, and promoting peer connectedness
- Promote community engagement activities e.g., religious activities, community clean-up and greening activities, and group physical exercise
- Train teachers, coaches, clergy, emergency responders, primary and urgent care providers, to identify people who may be at risk of suicide and to respond effectively
Teen Birth
- Encourage teens not to have sex
- Recognize long-acting reversible contraception (LARC) as a safe and effective first-line choice of birth control for teens
- Provide teens with knowledge about LARC and explore funding options to cover costs
- Offer a broad range of birth control options to teens, and discuss the pros and cons of each
- Seek training in LARC insertion and removal, have supplies of LARC available, and explore funding options to cover costs
- Remind teens that LARC by itself does not protect against sexually transmitted diseases and that condoms should also be used every time they have sex
- Talk with their teens about sex, including encouraging them not to have sex
- Encourage teens to use effective birth control to prevent pregnancy, along with condoms to protect against sexually transmitted diseases
- Visit a health care provider with the teen to learn about various types of birth control, including LARC
- Check with their health plan(s) about coverage of preventive services. Birth control and counseling may be available for teens at no out-of-pocket cost
- Locate Title X-funded centers for possible financial help
- Use educational campaigns to encourage teens not to have sex
- Licensed and accredited child care facilities are available where needed
- Availability of preschool enrichment with family engagement programs that provide parents social support, educational opportunities, and access to community resources.
- Subsidized child care
- State and federal earned income tax credit
- Section 8 housing
- SNAP benefits
- Livable wages
- Paid leave
- Flexible and consistent schedules
Violent Crime
According to the Community Preventive Services Task Force, (CPSTF) primary prevention interventions to reduce perpetration of intimate partner violence and sexual violence among youth, may be implemented in schools (middle school, high school, or college), at home, in communities, or in a combination of settings.
They may target groups at high risk for violence or the general population, both of which may include youth who have already experienced intimate partner violence or sexual violence as a victim or perpetrator.
- Teaching healthy relationship skills
- Promoting social norms that protect against violence
- Creating protective environments
- Interventions that taught healthy relationship skills OR promoted social norms to protect against violence reported favorable and consistent decreases in perpetration.
- Interventions that taught healthy relationship skills OR combined teaching healthy relationship skills with efforts to promote social norms that protect against violence, reported favorable and consistent decreases in victimization.
- Interventions that used all three strategies in combination reported decreases in perpetration and victimization.
Interventions that promote social norms to protect against violence through bystander education and empowerment, engaging men and boys as allies in prevention, or both are also recommended.
Chronic absenteeism
- Prioritize the development of early warning prevention and intervention systems that identify students who are, or are at risk of becoming, chronically absent before they miss enough school that it is nearly impossible for them to catch up
- Focus on developing positive messages for youth and families as well as implementing supportive engagement strategies
- Launch local initiatives to raise public awareness about the causes and effects of chronic absenteeism, including awareness among families and youth
- Regularly communicate across sectors that chronic absenteeism is a problem that affects the whole community, not just those students who are chronically absent and their families
- Community collaboration such as Integrated Student Supports programs
- Parent / guardian engagement and home visits
- Mentoring: pairing a caring adult or older student with an at-risk youth
- Safe Passage Program: adult monitors are placed along the streets and paths around select schools
- Extended Learning Programs/Summer Learning Program
- Incentives including praise and public recognition or material / monetary rewards